The Push to Raise the Legal Age to Buy Tobacco to 21 Has Little Basis in Fact
Weak Associations and Disregard for Unintended Consequences Make for Bad Policy

The notion that raising the tobacco purchasing age to 21 helps reduce adolescent smoking seems plausible enough. But there is little evidence in support of the idea, despite how much traction it has gotten lately. Senate Majority Leader Mitch McConnell (R-Ky.) has announced plans to introduce legislation to raise the legal age for purchasing tobacco nationwide.[1] Yet, there is little evidence not only about the effectiveness of such a policy—known as tobacco21—but also about its possible unintended negative effects. Tobacco21 advocates do not appear bothered by these uncertainties. Worse, much of the supposed evidence they cite fails to stand up to scrutiny.
The Needham “Miracle.” Without scientific evidence about the effects of raising the tobacco age to 21, advocates instead point to anecdotes where tobacco21 seemingly worked, especially a case known as the Needham “Miracle.”[2] In 2005, Needham, Massachusetts, a small suburb of Boston, became the first town in the U.S. to set the tobacco purchasing age at 21. As the story goes, in the years that followed adolescent smoking rates in Needham declined dramatically and much more than in the towns surrounding Needham that maintained a tobacco purchasing age of 18. It may sound like a success, but the idea that raising the tobacco age limit to 21 caused these declines does not hold up to close inspection.
Those citing the Needham “miracle” often refer to a 2015 study authored by Jonathan Winickoff of Harvard, Shari Kessel Schneider of the public health nonprofit Education Development Center, and colleagues. After comparing Needham’s smoking rate to those in 16 other school districts between 2006 and 2012, the authors reportedly found that “from 2006 to 2010, the decrease in 30-day smoking in Needham … was significantly greater than in the comparison communities.” [3] They concluded that their results “suggest that raising the minimum sales age to 21 for tobacco contributes to a greater decline in youth smoking … [and] support local community-level action to raise the tobacco sales age to 21.”[4]
Careful readers will notice something odd about the reported results: The study analyzed data for 2006 to 2012, but the conclusion only draws upon data from 2006 to 2010. Why? Reading beyond the paper’s abstract, one notices this important passage:
From 2006 to 2008, current smoking decreased at a greater rate in Needham than in the comparison communities and again from 2008 to 2010. However, from 2010 to 2012, decreases in current smoking were significantly greater in the comparison communities than in Needham.[5] [Emphasis added]
In other words, the data only showed greater declines in smoking in Needham during the first four years after it implemented tobacco21. Two years later, however, Needham’s reductions were less than in the neighboring towns that kept the tobacco age limit at 18. The last two years’ worth of data did not indicate that tobacco21 works; the study’s authors simply ignored it. Unfortunately, news media, anti-smoking advocates, and even some researchers continue to cite the Needham experience as proof that tobacco21 reduces adolescent smoking.[6]
Does Needham Refute Tobacco21? A careful look at all the data, from 2006 to 2012, indicates that Needham’s declines in adolescent smoking were far from miraculous. They were not even better than in the nearby towns that kept the tobacco age limit at 18. So does this disprove the effectiveness of tobacco21? No, but it does not prove that tobacco21 works, either. And more recent survey data do not help tobacco21 advocates. Compared to Needham, the declines in smoking were even lower in the surrounding towns.
A biennial survey conducted by the MetroWest Health Foundation includes health data for high school students in schools in the area of Massachusetts served by MetroWest—primarily the Boston area.[7] While MetroWest publishes the region-wide data after every survey, district-specific data are only made public at the discretion of the school districts or local health boards. But data for four neighboring towns are publicly available, in addition to Needham: Ashland, Medfield, Wayland, and Westborough.[8]
Looking at the changes in current smoking among these towns, we can see by 2014 that Needham’s declines were significantly outpaced by the others. Since 2006, the rate of current smoking among Needham high school students had declined by 40 percent, while the rates in the other towns declined by 59 to 77 percent.
By 2016, the other towns, except Westborough, joined Needham in raising the age limit for tobacco to 21. But the smoking rates in these towns did not suddenly decrease as happened in Needham. In fact, the rate of current smoking in all of these towns increased.
Opponents of tobacco21 might argue that the spike was caused by the age limit increase, and that some studies lend credibility to that idea as restrictions on rarer forms of nicotine consumption, such as e-cigarettes, tend to push people toward combustible cigarettes, which are the most widely available tobacco product.[9] Tobacco21 advocates could point out that Needham was the only town that did not see a spike in youth smoking between 2014 and 2016. But neither argument is particularly convincing. One year’s worth of data doesn’t tell us much and it is hard to conclusively prove how the 21 age limit prevented a spike in smoking in Needham when all of the other towns, except Westborough, had imposed the same age limit by 2015.
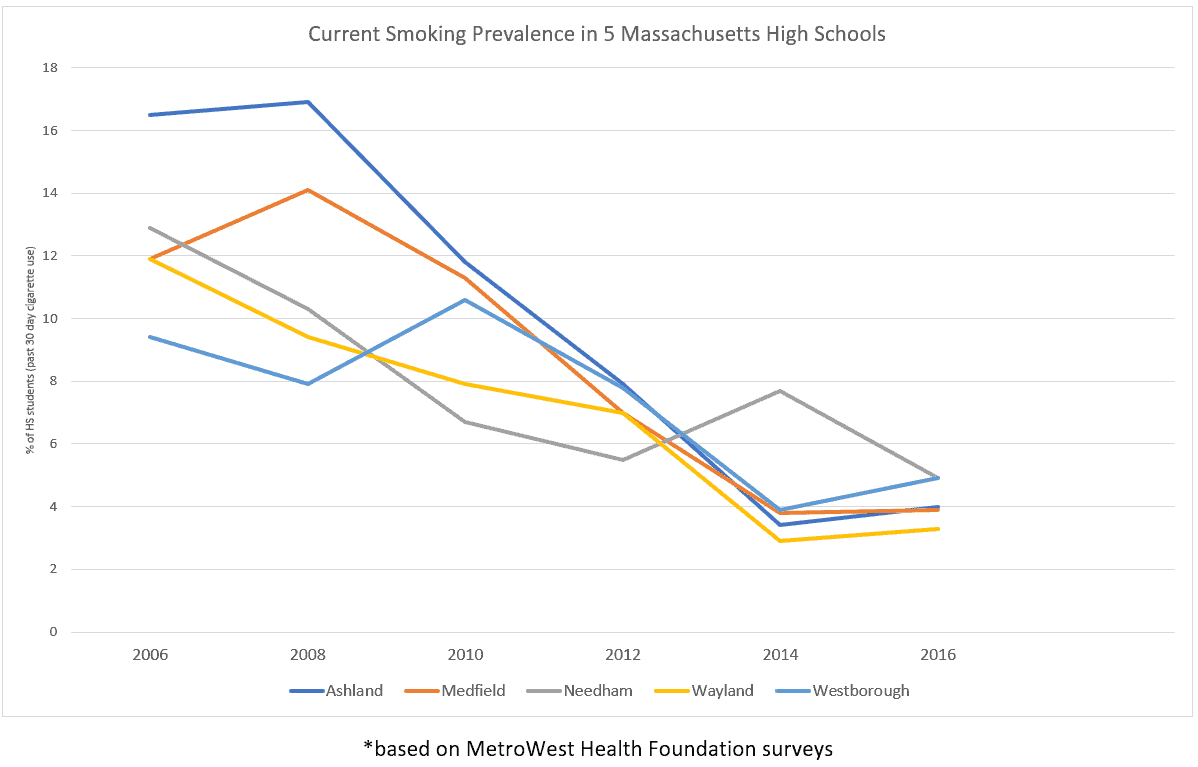
Looking at one or a few years of pure data rarely captures the whole story, but by comparing Needham’s smoking rates with neighboring towns that did not raise the tobacco age limit to 21—using all the years for which there is data—does show that the age limit of 21 did not lead to Needham’s smoking rates declining more than in other towns. Needham’s 2016 rate of current smoking was 4.9 percent, exactly the same as that of Westborough, which maintained a tobacco age limit of 18. Both had the highest prevalence of smoking all the five towns. Yet, the authors of the Needham study chose to draw their conclusion based on a shorter time period than that for which they had data available, for no discernible reason.
What Does It Mean? All of this means that tobacco21 might help or it might hurt adolescent smoking rates—but the Needham experience doesn’t tell us one way or the other. It seems unlikely that the age limit for purchasing tobacco had very much to do with the declines or increases in adolescent smoking observed in Needham or in any of the towns around it.
However, it raises some questions about the effectiveness of tobacco21. While it seems unlikely that tobacco21 advocates will stop citing Needham as evidence that tobacco21 works, we can hope that members of Congress will have the good sense to require a rigorous study of the policy before implementing it across the nation.
Notes
[1] Sasha Ingber, “Anti-Tobacco Advocates Question McConnell Plan To Raise Minimum Purchasing Age,” National Public Radio, April 19, 2019, https://www.npr.org/2019/04/19/715117833/anti-tobacco-advocates-question-mcconnell-plan-to-raise-minimum-purchasing-age.
[2] American Heart Association, “Vaping ignites legislative trend: Raising sales age for tobacco to 21,” American Heart Association News, May 30, 2019, https://www.heart.org/en/news/2019/05/30/vaping-ignites-legislative-trend-raising-sales-age-for-tobacco-to-21.
[3] Shari Kessel Schneider, Stephen L. Buka, Kim Dash, Jonathan P. Winickoff, Lydia O’Donnell, “Community reductions in youth smoking after raising the minimum tobacco sales age to 21,” Tobacco Control, Vol. 25, Issue 3 (2016), pp. 355-359, https://tobaccocontrol.bmj.com/content/25/3/355.
[4] Ibid.
[5] Ibid.
[6] Matt Rocheleau, “Smoking among Needham high schoolers plunged after legal age rose to 21,” Boston Globe, June 17, 2015, https://www.bostonglobe.com/2015/06/17/smoking-among-needham-high-schoolers-plunged-after-legal-age-rose/k0KDLz110EWI7W7TxCtOXJ/story.html. American Heart Association, “Vaping ignites legislative trend.” Micah L. Berman, “Raising the tobacco sales age to 21: surveying the legal landscape,” Public Health Reports, Vol. 131, No. 2 (2016), pp. 378-381, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4765989.
[7] Foundation Publications, MetroWest Health Foundation, https://www.mwhealth.org/Learning-Insights/Foundation-Publications#68438-adolescent-health.
[8] MetroWest Adolescent Health Surveys available for Needham, http://www.needhamma.gov/index.aspx?NID=4113; Ashland, https://www.ashlanddecisions.org/wp-content/uploads/2018/10/2016-MWAHS-Full-Report-ASHLAND-High-School.pdf; Medfield, http://www.medfield.net/district-information/metrowest-health-survey-results; Wayland, https://www.wayland.k12.ma.us/UserFiles/Servers/Server_1036352/File/District/Main%20Page%20Docs/2016%20MWAHS%20Highlight%20Report%20-%20WAYLAND%20High%20School.pdf; Westborough, https://www.town.westborough.ma.us/sites/westboroughma/files/uploads/2016_mwahs_westborough_key_indicator_report.pdf.
[9] Abigail Friedman, “How does electronic cigarette access affect adolescent smoking?” Journal of Health Economics, Vol. 44 (2015), pp. 300-308, https://www.ncbi.nlm.nih.gov/pubmed/26583343. Michael F. Pesko, Jenna M. Hughes, Fatima S. Faisal, “The influence of electronic cigarette age purchasing restrictions on adolescent tobacco and marijuana use,” Preventative Medicine, Vol. 87 (2016), pp: 207-212, https://www.sciencedirect.com/science/article/pii/S0091743516000396.