Congress gets into the PBM business

Photo Credit: Getty
In the recently passed appropriations bill, Congress enacted several Pharmacy Benefit Manager (PBM) reforms it has been contemplating for years. On the surface, these reforms appear reasonable, but on closer examination, they will likely do nothing or even harm consumers.
Many members of Congress, policy wonks, and other participants in the health care sector all argue that PBMs drive up drug prices, distort the market, block treatments, and profit enormously. Dig below the surface though, and the broad evidence — not cherry-picked anecdotes or unrepresentative cases — tells a different story.
Drug prices rising slowly
While the eye-popping prices of certain brand-name drugs receive many of the headlines, average prices show a less dramatic story. Over the past 10 years, when PBMs were purportedly a highly concentrated industry with myriad abuses, the price of prescription drugs rose more slowly than average prices did, and much more slowly than all medical care.
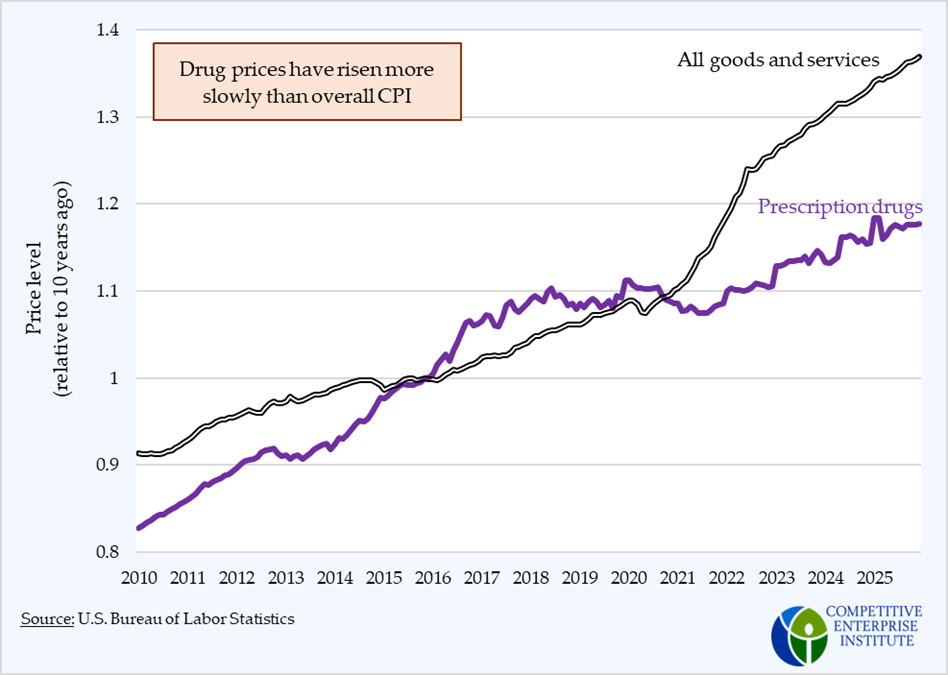
This is largely due to a shift from brand-name drugs to generics. Brand-name drugs that command the highest prices are always on the clock. Eventually the patent expires and competition with generics brings those drugs to the public for much lower prices. This is why Amazon can offer an unlimited supply of certain drugs for $5/month; drugs that would have cost hundreds of dollars 20 years ago.
Misconceptions about drug prices have driven Congress to prescribe a specific structure for PBM contracts, one that puts the preferences of Congress and other stakeholders above consumer choice and welfare.
De-linking
The bill demands several changes in different markets. In Medicare, Congress is prohibiting compensation structures tied to drug list prices. This is called de-linking. Again, on the surface, there appear to be reasonable justifications for this. For one, PBMs often don’t themselves pay the list price for these drugs. They negotiate rebates from drug manufacturers. In effect, PBMs are paid full price for the drugs even when they negotiate rebates. This, many argue, creates distorted incentives for PBMs to favor drugs with higher list prices, which could increase costs for taxpayers and enrollees. The evidence supporting this claim is pretty thin, predominantly reliant on anecdotes. Findings from the Government Accountability Office suggest that PBMs already pass on 99 percent of these rebates to plan sponsors, i.e., insurance companies or other payers. Because rebates account for such a small portion of revenues, the opportunity for distortions in the market for prescription drugs is similarly small.
However, one should also consider the implications of this law beyond the first-order change in payment structure. Some argue this will drive down PBMs’ incentive to extract these rebates from the drug companies. To the extent that these rebates were making their way to consumers in the form of lower premiums, preventing them will tend to raise premiums. And there is a lot of evidence that this chain of events was occurring both in Medicaid and Medicare.
The following chart, taken from the 2025 MedPAC report linked above, shows how premiums for prescription drug plans have fallen, and remain lower than they were in 2018 despite a small uptick in 2024. This trend contrasts with nearly all other health care costs, and even general prices.

Also, PBM profit margins are comparable to those of independent pharmacies. OptumRx and ExpressScripts’ recent margins were both around or under 4 percent. CVS Caremark doesn’t provide PBM-specific margins. Independent pharmacies, in general, can expect around a 3 percent net profit margin.
Pass-throughs
Another provision in the bill concerns the rebates that drug manufacturers offer on certain drugs. The bill requires that they be passed on directly to employers who are purchasing the PBMs’ services. This is a direct intrusion into market forces. In a functioning market, this will happen naturally, as a product of competition between PBMs fighting to gain the employers as customers. To reiterate, the profit margin data and experience in public insurance programs suggest that competition is already occurring and the rebates are being passed through. There’s little evidence that PBMs are systematically pocketing these rebates to pad their bottom lines. Low profit margins demonstrate how unnecessary the massive intrusions Congress wants to make into this industry are. They also suggest that Congress isn’t trying to fix a problem with the market, but a problem with political perception.
The drug supply chain is one of the most complex industries in the economy, yet Congress wants to micromanage how it works, blocking some organizational and payment structures to favor others. Congress can’t balance its own budget and hasn’t passed a timely budget in a generation, yet they believe they can better manage the drug industry than the market. They can’t. Their bill will have negative unintended consequences and will put the benefits consumers have enjoyed over the past 20 years — transition to generics, lower overall costs, and newer medicines — at risk.